How Mental Health Triage Works: A Clear Parent's Guide
- joeudesign
- May 24
- 10 min read

TL;DR:
Mental health triage involves a multi-step process assessing safety, emotional impact, and support needs to direct individuals to appropriate care swiftly. Pediatric triage is often inaccurate, with over- and under-triage impacting children and highlighting disparities, so parental advocacy and documentation are vital for better outcomes. Post-triage, personalized safety plans and timely follow-up care—often via telehealth—are essential for preventing repeated crises and promoting stability.
When your child is struggling or you are facing your own mental health crisis, the last thing you want is confusion about what happens next. Understanding how mental health triage works can mean the difference between hours of uncertainty and getting to the right level of care quickly. Triage is far more than a quick risk check. It is a structured workflow that matches people to the care they actually need, from a phone call with a crisis counselor to an in-person psychiatric evaluation. This guide breaks down every step in plain language, with special attention to pediatric triage and practical advice for parents.
Table of Contents
Key Takeaways
Point | Details |
Triage is a dynamic process | Mental health triage is a multi-step workflow, not a single risk label assigned at intake. |
Pediatric triage has accuracy gaps | Studies show triage is inaccurate in two-thirds of pediatric cases, often erring toward over-triage. |
Safety planning follows triage | After initial screening, counselors and clinicians create personalized safety plans with concrete coping strategies. |
Geography shapes your options | Triage models vary by location, with telehealth and mobile crisis teams expanding access across New York State. |
Parental advocacy changes outcomes | Parents who communicate detailed safety information during triage significantly improve accuracy and care routing. |
How mental health triage works: the core workflow
Most people picture triage as a single question: “Is this person safe right now?” In reality, the mental health assessment process involves several distinct, sequential steps. Each one builds on the last, and skipping a step can mean the wrong level of care.
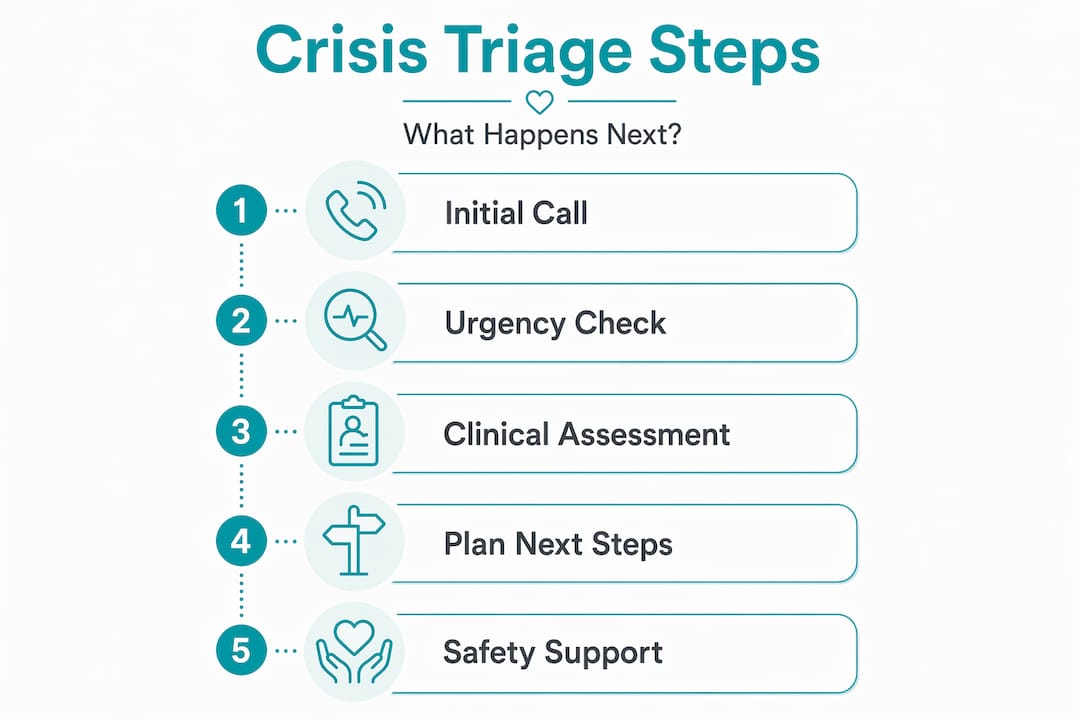
Here is how a typical triage system for mental health unfolds:
Initial contact. A person reaches out by phone, text, or chat. The 988 Suicide and Crisis Lifeline is the most common entry point in the United States, but crisis centers, hospital emergency departments, and outpatient clinics each have their own intake processes.
Immediate safety screening. Counselors ask direct safety questions early in the call to guide real-time risk assessment. This is not just supportive listening. It is structured screening with specific questions about suicidal thoughts, plans, and access to means.
Emotional health and problem impact assessment. Beyond safety, the counselor or clinician evaluates how severely the person’s symptoms are affecting their daily functioning. This includes sleep, work or school performance, relationships, and recent escalation in distress.
De-escalation and stabilization. Once the immediate risk picture is clearer, the focus shifts to calming the person, reducing acute distress, and building a shared understanding of what support is needed.
Safety plan creation. Triage counselors engage in safety plan creation, which involves identifying coping strategies, trusted contacts, and steps to restrict access to lethal means. A safety plan is not a contract. It is a concrete, personalized tool.
Disposition planning. This is where triage separates risk screening from the next steps. After ruling in or out imminent danger, workflow shifts toward crisis resolution and routing. Options include mobile crisis teams, emergency department referral, telehealth follow-up, or community-based outpatient services.
Triage is a dynamic workflow that distributes people to the care they need while minimizing delays and reducing unnecessary hospitalization. Understanding that distinction between risk screening and disposition planning helps you ask better questions and advocate more effectively for yourself or your child.
Pro Tip: If you are calling 988 for the first time, prepare to answer direct questions about safety, suicidal thoughts, specific plans, and access to means. The more detail you provide, the more accurately the counselor can route you to the right level of care.
Pediatric triage: what parents need to know
Children and adolescents do not experience or express mental health crises the same way adults do. Their symptoms can look like behavioral problems, school refusal, or sudden emotional outbursts that adults sometimes dismiss. This communication gap has real consequences inside the triage system.

Research published in 2026 found that pediatric triage is inaccurate in two-thirds of emergency department cases. Over-triage, meaning children are assigned a higher acuity level than their condition warrants, occurs in 57% of cases. Under-triage, the more dangerous error where a child’s severity is underestimated, happens in 8% of cases. Both patterns cause harm. Over-triage leads to longer waits, more invasive interventions, and unnecessary stress for families. Under-triage can mean a child in genuine crisis does not get the prompt psychiatric attention they need.
Disparities are also documented by race, ethnicity, and language preference. Equity gaps in pediatric triage can be addressed through staff training on implicit bias and improved language services, but many facilities have not yet made those changes. If English is not your family’s primary language, request a medical interpreter at the start of any triage encounter.
Here is what parents can do to improve outcomes during the mental health assessment process for a child:
Bring written documentation. Note your child’s recent symptoms, any previous mental health diagnoses (such as ADHD, anxiety, OCD, or autism spectrum disorder), current medications, and any recent changes in behavior.
Speak directly about safety. Parents who communicate clearly about suicidal thoughts, self-harm, or access to means help counselors make more accurate routing decisions.
Request reassessment if the situation changes. Changes in patient behavior after triage warrant a new evaluation rather than accepting the initial severity determination as final. If your child’s agitation increases or suicidal thoughts persist after triage, tell a staff member immediately.
Ask what level of care is being recommended and why. You have the right to understand the reasoning behind any disposition decision.
“Parents and patients benefit from understanding triage stages so they can better communicate during assessment calls and improve outcomes for the people they love.”
Connecting a child in crisis to child and adolescent psychiatry services, rather than a general emergency environment, often leads to faster stabilization and a more appropriate follow-up plan. Knowing how to advocate during triage makes that connection more likely.
Triage models: how settings and regions differ
Not all triage systems look the same, and geography matters more than most people realize. How you evaluate mental health crises depends heavily on where you are, what time it is, and what services your region has invested in.
The table below shows the key differences between common triage models:
Triage model | How contact happens | Response type | Best suited for |
988 telephone triage | Phone, text, or chat | Crisis counselor, safety planning, referral | Any level of crisis, initial contact |
Emergency department triage | In-person | Nurse or clinician assessment, possible hospitalization | Acute or high-risk situations |
Mobile crisis team | Dispatched to location | Mental health professionals on-site | Community-based rapid response |
Telehealth psychiatry | Video or phone | Ongoing psychiatric follow-up and medication management | Post-crisis and ongoing care |
Mobile crisis teams staffed by mental health professionals provide rapid, trauma-informed community response including de-escalation, safety planning, and referrals as alternatives to hospitalization and law enforcement involvement. These teams are increasingly dispatched directly through 988, particularly for situations where someone needs support but not emergency medical care.
Geographic routing is a real and sometimes overlooked part of how triage functions. In some models, a caller’s home address determines whether they are connected to metropolitan or rural acute services. This means two people experiencing a similar level of distress may receive very different responses based purely on location.
In New York, telehealth psychiatry services have significantly expanded access for people in Westchester County and beyond. A person who completes telephone or video triage can be connected to ongoing psychiatric care without traveling to a facility, which reduces the gap between crisis stabilization and sustained treatment.
Effective crisis care systems include someone to contact, someone to respond in the community, and a safe place for immediate stabilization. Understanding which of these three elements you are accessing at any given moment helps you know what to expect and what to ask for.
Safety planning and follow-up care after triage
Triage is the beginning of the care pathway, not the end. What happens in the days after an initial crisis contact determines whether someone stays stable or cycles back into crisis.
Effective safety plans go beyond a phone number on a card. Safety plans involve concrete coping strategies and means restriction to reduce suicide risk. They include identifying specific trusted contacts, naming warning signs that signal escalating distress, and listing grounding strategies that work for that particular person. For children, this plan should include a school counselor or trusted teacher if school refusal or behavioral issues are part of the picture.
After triage, the follow-up pathway typically includes these components:
Psychiatric follow-up appointment. Scheduling this within 24 to 72 hours of a crisis contact dramatically reduces the risk of re-crisis. This is where medication management may begin or be adjusted for conditions like anxiety, depression, ADHD, or OCD.
Connection to ongoing therapy. Triage identifies the level of care, but therapy provides the ongoing support structure. Cognitive behavioral approaches and family therapy are frequently recommended after pediatric mental health crises.
Coordination between providers. When a person has multiple conditions, such as autism spectrum disorder alongside anxiety, coordination between the psychiatrist, therapist, and primary care provider improves outcomes significantly.
Postpartum and perinatal mental health monitoring. New mothers who come through triage need specific follow-up pathways. Postpartum depression and anxiety require different medication management considerations and ongoing support beyond a single triage encounter.
Insurance and access verification. Before leaving any triage encounter, confirm that your next appointment is covered under your insurance plan. Most psychiatric practices in New York, including those offering telehealth services statewide, accept a wide range of insurance plans.
Pro Tip: After any mental health crisis intervention, write down the name of the counselor or clinician who created your safety plan and ask for a copy before you leave or end the call. Having it in writing makes follow-up care much more effective.
Studies show 988 Lifeline callers often feel less depressed, less suicidal, and more hopeful after speaking with a crisis counselor. That outcome is not accidental. It reflects a well-designed triage process that combines risk screening, emotional support, and clear next steps. The addiction recovery pathway often follows a similar post-crisis structure, emphasizing that stabilization is only meaningful when it connects to sustained care.
My perspective on triage effectiveness and what it misses
I have spoken with many families in New York who came away from an emergency triage experience feeling more confused than when they arrived. They were told their child was “low risk” and sent home with a phone number. Days later, the crisis returned. That experience is not a failure of triage as a concept. It is a failure of how triage is too often applied in practice.
What I have observed is that triage gets treated as a one-time determination when it should be treated as an ongoing assessment. The moment a child’s symptoms shift after discharge, the clock should reset. Initial severity determinations are not permanent, and families should feel empowered to say so.
I have also seen how much parental preparedness changes the trajectory. When a parent walks into an emergency department or calls 988 with a clear account of their child’s recent behavior, medication history, and specific safety concerns, the triage counselor can work faster and more accurately. That preparation is not about being a medical expert. It is about knowing your child and communicating what you know with confidence.
The equity gaps in pediatric triage trouble me deeply. Non-English-speaking families and children from marginalized communities are at higher risk of receiving inaccurate triage determinations. Clinically excellent triage requires culturally sensitive training and language access. Until that becomes standard, advocacy matters even more.
Telehealth psychiatry has genuinely improved what happens after triage for many of my patients in New York, particularly those in Westchester County who previously had limited access to specialized child and adolescent psychiatry. Timely medication management through a telehealth appointment has, more than once, prevented a second crisis within the same week.
— Martin
Get the right psychiatric support after triage
Understanding triage is one thing. Getting connected to consistent, personalized psychiatric care is the step that truly changes lives.
At 2ndarc, we specialize in child and adolescent psychiatry, adult psychiatry, and telehealth services across New York State, including White Plains and Brooklyn. Whether your family is navigating the aftermath of a mental health crisis or seeking support for anxiety, depression, ADHD, OCD, autism spectrum disorder, or postpartum mental health, we create individualized treatment plans built around your specific needs. Most major insurance plans are accepted, and appointments are often available within 24 hours. Telehealth options make care accessible across New York without the stress of travel.
Ready to take the next step? Book your consultation today and connect with a compassionate psychiatric team that listens, collaborates, and supports you through every stage of care. You can also visit 2ndarc.com to learn more about our services and what to expect from your first appointment.
FAQ
What is mental health triage?
Mental health triage is a structured process that evaluates a person’s safety, emotional health, and support needs to route them to the most appropriate level of care. It includes risk screening, de-escalation, safety planning, and disposition, and it can occur by phone, in person, or through telehealth.
How accurate is pediatric mental health triage?
Research shows that pediatric mental health triage in emergency departments is inaccurate in approximately two-thirds of cases, with over-triage occurring in 57% and under-triage in 8%. Parents should advocate for reassessment if symptoms change after the initial evaluation.
What happens after mental health triage?
After triage, the next steps typically include a personalized safety plan, a scheduled psychiatric follow-up within 24 to 72 hours, and connection to ongoing therapy or medication management. The goal is to prevent re-crisis through continuous, coordinated support.
Can parents call 988 on behalf of their child?
Yes. Parents and caregivers can call 988 on behalf of a child in crisis. Providing clear, specific information about the child’s symptoms, safety concerns, and mental health history helps the counselor make a more accurate triage determination and connect the family to appropriate resources.
How does telehealth fit into the mental health triage system?
Telehealth psychiatry typically functions as a post-triage follow-up option rather than an acute crisis response. After initial stabilization, telehealth appointments allow people across New York State to access ongoing psychiatric care, medication management, and therapy without requiring in-person visits.
Recommended