How Psychiatrists Diagnose Depression: What to Expect
- joeudesign
- 2 hours ago
- 8 min read

TL;DR:
Psychiatrists diagnose depression through DSM-5-TR criteria, clinical interviews, standardized tools, and lab tests. They assess symptom severity, duration, and impact to distinguish depression from medical conditions and other mental disorders. Diagnosis varies across age groups, with telehealth expanding access and enabling thorough evaluations across New York State.
Depression is defined as a clinical condition in which a persistent pattern of low mood, loss of interest, and functional impairment meets specific diagnostic criteria established by the DSM-5-TR. Understanding how psychiatrists diagnose depression removes the uncertainty from the evaluation process and helps you walk into your first appointment with confidence. The process is not a simple checklist. It combines the DSM-5-TR framework, standardized tools like the PHQ-9, clinical interviews, mental status exams, and selective lab work to build a complete picture of what you are experiencing. Guidance from the Merck Manual confirms that diagnosis hinges on symptom presence, severity, duration, and real-world impact, not a single test or a single visit.
How psychiatrists diagnose depression: symptoms and criteria
The foundation of any depression diagnosis is the DSM-5-TR, the Diagnostic and Statistical Manual of Mental Disorders. To meet the criteria for major depressive disorder (MDD), at least five of nine symptoms must be present nearly every day during the same two-week period. At least one of those five must be either depressed mood or a loss of interest and pleasure in activities you once enjoyed.
The nine core symptoms psychiatrists evaluate include:
Depressed mood most of the day
Markedly diminished interest or pleasure in activities (anhedonia)
Significant weight loss or gain, or changes in appetite
Insomnia or sleeping too much
Psychomotor agitation or slowing that others can observe
Fatigue or loss of energy
Feelings of worthlessness or excessive guilt
Difficulty concentrating or making decisions
Recurrent thoughts of death or suicidal ideation
Beyond symptom count, the DSM-5-TR diagnostic criteria require that these symptoms cause significant distress or impairment in social, occupational, or other areas of daily functioning. A person who feels sad for a few days after a difficult event does not meet this threshold. The pattern must be persistent, pervasive, and disruptive to qualify as clinical depression.
Psychiatrists also distinguish between different depressive conditions. MDD involves discrete episodes, while persistent depressive disorder (dysthymia) involves a lower-grade but chronic depressed mood lasting at least two years. The symptom pattern, duration, and severity guide which diagnosis applies.
Pro Tip: Write down your symptoms before your appointment, including when they started, how often they occur, and how they affect your daily life. This kind of detail helps your psychiatrist apply the DSM-5-TR criteria accurately and saves valuable time during the evaluation.
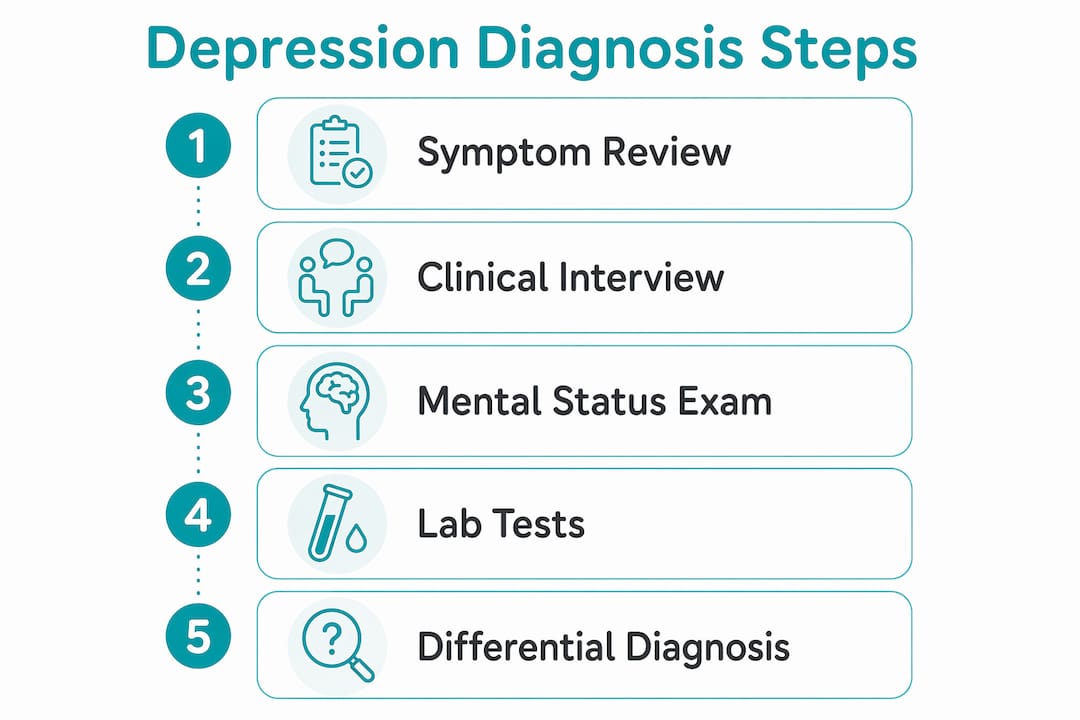
What does the clinical evaluation actually involve?
The clinical evaluation is where the psychiatrist diagnosis process goes beyond a symptom checklist. Structured clinical interviews combined with a mental status exam allow the psychiatrist to assess mood, cognition, behavior, and overall functioning in real time. This is not a passive process. Your psychiatrist is observing how you speak, your affect, your energy, and your thought patterns throughout the conversation.
A thorough evaluation typically follows this sequence:
Chief complaint and history of present illness. You describe what brought you in, when symptoms began, and how they have changed over time.
Psychiatric history. Prior episodes of depression, previous diagnoses, past medications, and any hospitalizations are reviewed.
Family history. A family history of depression, bipolar disorder, or other mood disorders raises the clinical index of suspicion.
Mental status exam. The psychiatrist assesses appearance, speech, mood, affect, thought content, cognition, and insight.
Safety assessment. Suicidal ideation is evaluated directly and compassionately as both a symptom and a risk factor. Safety planning is integrated into this step when needed.
Differential diagnosis. The psychiatrist rules out anxiety disorders, bipolar disorder, ADHD, OCD, and medical conditions that can mimic depression.
Ruling out bipolar disorder deserves special attention. Screening for manic episodes is a standard part of every depression evaluation because treating bipolar disorder with antidepressants alone can trigger a manic episode. If you have ever had periods of unusually high energy, decreased need for sleep, or impulsive behavior, your psychiatrist needs to know.
Comorbidities like anxiety and ADHD are common alongside depression and complicate the picture. The co-occurrence of depression and anxiety is well documented, and both conditions must be identified to create an effective treatment plan. Clinical judgment, not a checklist, is what separates an accurate diagnosis from an incomplete one.

What lab tests and physical exams support the diagnosis?
No laboratory test definitively diagnoses depression. That is one of the most important things to understand about the psychiatric evaluation process. Labs serve a different purpose: they exclude medical conditions that can produce depressive symptoms and would require a different treatment approach entirely.
Common tests ordered during a depression workup include:
Complete blood count (CBC): Rules out anemia, which causes fatigue and low mood
Thyroid-stimulating hormone (TSH): Hypothyroidism closely mimics depression
Electrolytes and metabolic panel: Identifies imbalances affecting mood and cognition
Vitamin B12 and folate levels: Deficiencies in both are linked to depressive symptoms
Testosterone (in older men): Low testosterone produces fatigue, low mood, and concentration problems
The table below summarizes what each test rules out and why it matters:
Lab Test | What it rules out |
TSH | Hypothyroidism mimicking depressed mood and fatigue |
CBC | Anemia causing low energy and cognitive slowing |
B12 and folate | Nutritional deficiencies producing mood and memory symptoms |
Electrolytes | Metabolic imbalances affecting brain function |
Testosterone (men) | Hormonal causes of fatigue and low motivation |
A physical exam may also be ordered to rule out neurological conditions like Parkinson’s disease, which can present with slowed movement, flat affect, and low mood. Lab results typically take a few days to return, which means diagnosis may span multiple visits when medical causes need to be excluded first. This is not a delay. It is the process working as it should.
Pro Tip: Follow through with every lab test your psychiatrist recommends, even if you feel confident the results will be normal. Ruling out a thyroid problem or B12 deficiency is not a formality. It protects you from receiving the wrong treatment.
How does diagnosis differ for children, teens, and adults in New York?
The core DSM-5-TR criteria apply across age groups, but the way depression presents and the factors that shape diagnosis vary significantly between children, adolescents, and adults. In pediatric and adolescent psychiatry, developmental factors and behavioral observations carry more diagnostic weight because younger patients often cannot articulate their internal experience the way adults can.
Children with depression may present with irritability rather than sadness, school refusal, physical complaints like stomachaches, or withdrawal from friends and activities. Adolescents often show increased sleep, academic decline, social isolation, and heightened emotional reactivity. These presentations can be mistaken for typical developmental behavior, which is why a trained child and adolescent psychiatrist is so important.
Comorbidities are especially common in younger patients. ADHD, anxiety disorders, autism spectrum disorder, and OCD frequently co-occur with depression in children and teens. Each condition influences how the others present, and an accurate diagnosis requires evaluating all of them together. A teen depression treatment plan must account for this complexity from the start.
For adults, postpartum and perinatal mental health adds another layer of diagnostic consideration. Postpartum depression is a distinct clinical presentation that requires specific screening and a tailored approach to medication management, particularly for breastfeeding patients.
Telehealth psychiatry has expanded access to evaluation across New York State significantly. Patients in Westchester County, White Plains, Brooklyn, and throughout the state can now complete initial assessments and follow-up visits through secure video appointments. This matters because many people experiencing depression face barriers to in-person care, including fatigue, transportation, and stigma. Telehealth removes those barriers without reducing the quality of the clinical evaluation.
Key takeaways
Comprehensive depression diagnosis combines DSM-5-TR criteria, clinical interviews, mental status exams, and targeted lab work to identify significant, persistent symptoms that impair daily functioning.
Point | Details |
DSM-5-TR is the standard | Five of nine symptoms for two weeks, including depressed mood or anhedonia, are required for an MDD diagnosis. |
Labs rule out mimics | Tests like TSH, CBC, and B12 exclude medical causes before a psychiatric diagnosis is confirmed. |
Bipolar screening is mandatory | Every depression evaluation includes a history of manic episodes to prevent misdiagnosis and unsafe treatment. |
Age shapes presentation | Children and teens often show irritability and school refusal rather than classic sadness, requiring adapted evaluation. |
Telehealth expands access | New York patients can receive full psychiatric evaluations via telehealth, removing barriers to timely care. |
What I’ve learned from watching patients navigate this process
The part of the diagnostic process that surprises people most is how much it depends on them. Psychiatrists rely heavily on patient self-report combined with clinical observation, and the quality of that self-report shapes everything that follows. Patients who minimize their symptoms, or who feel embarrassed to mention suicidal thoughts, often leave their first appointment with an incomplete picture on the table.
I have seen patients wait years for an accurate diagnosis because they described their worst days as “just stress” or never mentioned that they had stopped enjoying everything they used to love. The DSM-5-TR criteria are only as useful as the information fed into them. Your psychiatrist is not there to judge you. They are there to understand your experience clearly enough to help you.
The other thing worth saying plainly: a first appointment does not always produce a final diagnosis. When comorbidities like anxiety, ADHD, or bipolar disorder are in the picture, or when lab results are pending, the process takes more than one visit. That is not a failure of the system. It is the system protecting you from a rushed conclusion. A diagnosis that takes three visits and gets it right is worth far more than a diagnosis made in twenty minutes that misses something important.
If you are in New York and wondering whether what you are feeling qualifies as depression, the most useful thing you can do is start the treatment process with a qualified psychiatrist rather than waiting for certainty on your own. Certainty comes from the evaluation, not before it.
— Martin
Get a personalized depression evaluation at 2ndarc
If you have been experiencing signs of clinical depression and want to understand what is happening, 2ndarc is here to help. 2nd Arc Psychiatric Associates serves patients across New York with in-person appointments in White Plains and Brooklyn, as well as statewide telehealth psychiatry for those who prefer to be seen from home.
The 2ndarc team provides personalized evaluations for depression, anxiety, ADHD, OCD, and other mental health conditions for both adults and children. Most major insurance plans are accepted, and appointments are often available within 24 hours. Whether you are an adult navigating depression for the first time or a parent concerned about your teenager, the team at 2ndarc will listen, evaluate thoroughly, and work with you on a plan that fits your life. Book your consultation online today and take the first step toward feeling like yourself again.
FAQ
What does a psychiatrist ask during a depression evaluation?
Psychiatrists ask about the duration and severity of your symptoms, how they affect your daily life, your personal and family psychiatric history, and whether you have had any thoughts of self-harm. They also screen for conditions like bipolar disorder and anxiety that can overlap with depression.
How long does it take to get a depression diagnosis?
Diagnosis may occur at the first appointment if the symptom presentation is clear, but complex or comorbid cases often require additional visits. Lab results, which can take a few days, may also influence the timeline.
Can depression be diagnosed without a lab test?
Yes. No lab test confirms depression. Lab work excludes medical causes like thyroid disorders or B12 deficiency that mimic depressive symptoms, but the diagnosis itself is based on clinical criteria and evaluation.
What is the PHQ-9 and how is it used?
The PHQ-9 is a standardized screening tool that measures the severity of nine depressive symptoms. Psychiatrists use it to track symptom changes over time, but it does not replace a full clinical assessment for diagnosis.
Can children and teens be diagnosed with depression the same way as adults?
The DSM-5-TR criteria apply to all age groups, but developmental factors shape how symptoms present in younger patients. Children may show irritability and school refusal rather than sadness, and comorbid conditions like ADHD are more common, requiring a more adapted evaluation approach.
Recommended
Comments